HISTOPATHOLOGICAL STUDY OF NON-NEOPLASTIC LESIONS OF NOSE, PARANASAL SINUSES AND NASOPHARYNX
Original Article
Shah H, Baviskar BP, Dongre SD
Department of Pathology, Rural Medical College, Pravara Institute of Medical Sciences (PIMS), Loni, Maharashtra, India.
Correspondence: Shah H, Department of Pathology, Rural Medical College, Pravara Institute of Medical Sciences (PIMS), Loni, Maharashtra, India. E-mail: harsh25388@yahoo.co.in
ABSTRACT
Background: The various lesions of the nose, paranasal sinuses and nasopharynx were subjected to histopathological evaluation over a period of 5 years (2010 to 2015) at the Department of Pathology, in a rural-based hospital. Total of 84 specimens was studied over the time of 5 years. Methodology: The formalin-fixed specimens were received with complete clinical and radiological features. Routine gross examination and the required number of sections were taken and stained with hematoxylin and eosin. Result: In the study, 84 cases were of Inflammatory and Non-neoplastic lesions. Nasal polyps were the most common lesions with 77 (91.67%) cases. Among the all Nasal polyps, 77 cases, 20 (25.97%) cases were of Allergic polyp, 50 (64.93%) cases were of the inflammatory polyp, while 7 (9.09%) cases were of Antrochoanal polyp. 2 cases (2.38%) each of Sinusitis and Intradermal naevus. Rhinosporidiosis, Mucocele and Nasolabial cyst comprised of 1 (0.77%) case each respectively. Conclusion: In our study, the most common lesions were Nasal Polyps. Most of the cases were presented in 2ndand3rddecade of life with Male preponderance. Nasal obstruction was the most common clinical presentation in the present study.
Keywords: Nose; Paranasal sinuses; Nasopharynx; Non-Neoplastic Lesions.
INTRODUCTION
We perceive our environment through our sensory receptors like the nose. Tumours arising or involving nasal cavity and paranasal sinuses were recognized in the time of Hippocrates who distinguished between hard and soft tumours and also believed that treatment shortened the patient's life! [1].
The nasal cavity comprises of anterior and posterior part, paranasal sinuses and nasopharynx. The nasopharynx is notably the most difficult region to examine and there remain areas which may escape otolaryngologist’s routine and more detail examination [2]. Clinically and radiologically benign and malignant lesions are hard to differentiate. The only definitive method is biopsy [3].
A variety of non-neoplastic lesions involve nasal cavity, paranasal sinuses and nasopharynx [4].
Polyps are tumour like lesions in the nose which are projections of mucous membrane and develop in association with chronic rhinitis and sinusitis. Clinically polyps are smooth, shiny and present as movable swelling. It is quite impossible to distinguish clinically between simple nasal polyp, polypoidal lesions which are caused by specific granulomatous disease and polypoidal neoplasms [5]. Classification of tumours and tumour like lesions of the nasal cavity, paranasal sinuses and nasopharynx: Malformations, Inflammatory diseases, Benign tumours and Malignant tumours [6].
MATERIAL AND METHODS
Study design: Descriptive study.
Ethics approval: The study was approved by the IEC PIMS (DU).
Study place: The study was conducted in the Department of Pathology at Rural Medical College and Pravara Rural Hospital, Loni.
Study period: Over a period of 5 years (2010-2015).
Sample size: Total number of cases was 84.
Inclusion criteria: All specimens of lesions of Nose, Paranasal sinuses and Nasopharynx received in the Department of Pathology for Histopathological findings.
Collection of sample: All specimens were collected through Departments of ENT and Surgery from Operation Theatre and transported to the Department of Pathology, Rural Medical College, Loni, in 10% Formalin.
Methodology: Clinical data such as the age, sex, complaints and the record of other investigations were obtained from the patient. Biopsies of specific sites were received and then processed in the laboratory by routine processing and stained by H&E.
These lesions were evaluated on Haematoxylin & Eosin stained sections of paraffin-embedded 10% buffered formalin fixed tissue blocks.
Statistical analysis: Data were tabulated and presented in the form of a percentage.
RESULTS
In the present study, the highest incidence of Inflammatory and Non-neoplastic cases was in the 2nd, 3rd and 4th decade of life which were 16, 22 and 16 cases respectively. There were 4 cases in a 1st decade, 10 cases in the 5th decade, 6cases in the 6th decade, 9 cases in the 7th decade and 1 case in the 8th decade of Inflammatory and Non-neoplastic lesions. (Fig 1)
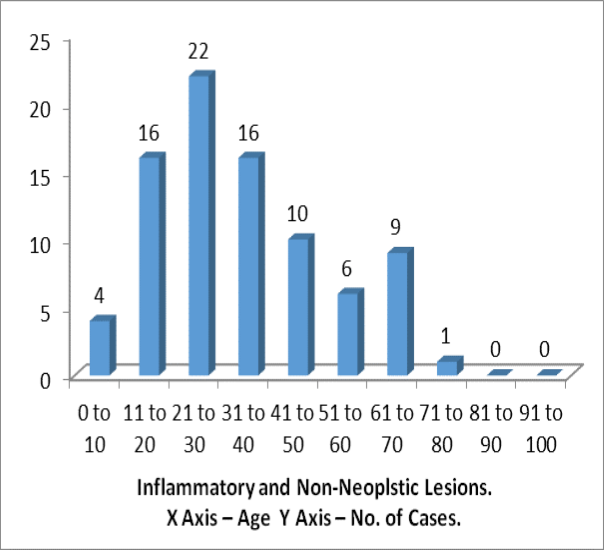
Fig 1. Age Wise Distribution of Inflammatory and Nonneoplastic Lesions
In the present study, Male (44) to female (40) ratio among Inflammatory and Non-neoplastic Lesion was 1.1:1. In the present study, the commonest complaint patient presented with was nasal obstruction. Out of 84 cases received, 68 (80.95%) complained of nasal obstruction. The second most common complaint was running nasal mass, 08 (9.52%) cases, followed by sneezing 5 (5.95%) and nasal discharge 3 (3.57%). (Fig 2)
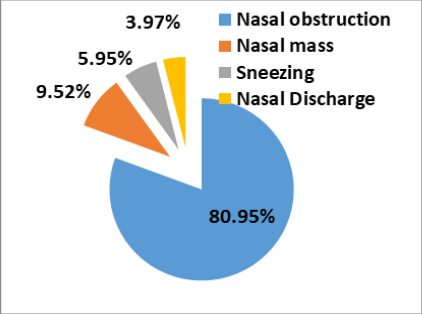
Fig 2. Distribution of Complaints of Patients
In the present study, a total of 84 cases was of Inflammatory and Non-neoplastic lesions. Nasal polyps were the most common lesions with 77 (91.67%) cases, followed by the 2 cases (2.38%) each of Sinusitis and Intradermal naevus. Rhinosporidiosis, Mucocele and Nasolabial cyst comprised of 1 (0.77%) case each respectively (Fig 3).
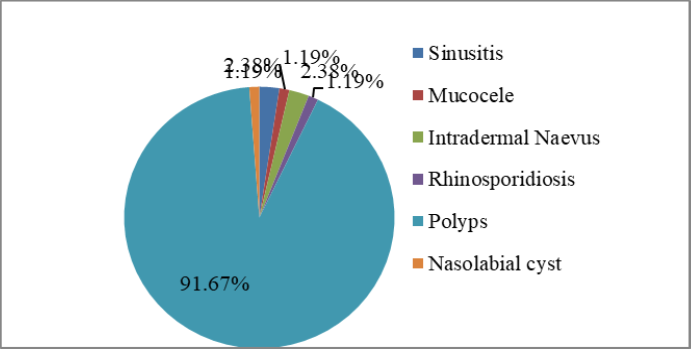
Fig 3. Distribution of Non-neoplastic lesions according to histologic findings.
Among the all Nasal polyps, 77 cases, 20 (25.97%) cases were of Allergic polyp, 50 (64.93%) cases were of the inflammatory polyp, while 7 (9.09%) cases were of Antrochoanal polyp (Table 1).
Table 1. Distribution of Nasal Polyp According to Histologic Findings.
|
Nasal Polyp |
No.of Cases |
% Cases |
|
Allergic polyp |
20/77 |
25.97 |
|
Inflammatory polyp |
50/77 |
64.93 |
|
Antrochoanal polyp |
07/77 |
9.09 |
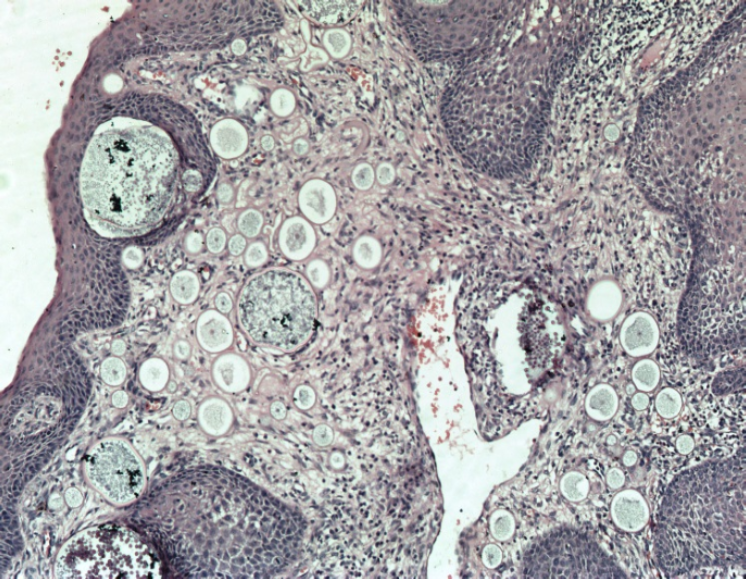
Fig 4. Rhinosporidiosis (H & E, X100)

Fig 5. Allergic Polyp (H & E, X400)
DISCUSSION
Histopathological examination is a simple and reliable diagnostic procedure for the detection of various lesions of the nasal cavity, nasopharynx and paranasal sinuses as most of the lesions are either inaccessible for fine needle aspiration cytology (FNAC).
In the present study, the total number of cases was 84 and the duration of the study was 5 years. An average number of cases per year in the present study was 17.4 cases/year. This finding matches with the study of Dasgupta A [7] with 17.5 cases/year, Kulkarni A [8] with 14.4 cases/year and Zafar U [4] with 20.5 cases/year.
In the present study, the age distribution in non-neoplastic cases was between 1st to 8th decades, peak achieving in 2nd, 3rd and 4th decades. These findings correlate with the findings of Biswas G et al [9], where peak incidence was in 1st and 2nd decades of life, Lathi A et al [10], where peak incidence was in 2nd, 3rd and 4th decades of life and in the study of Zafar U et al [4], where peak incidence was in 1st, 2nd and 4th decades.
In the present study, the male to female ratio was 1.1:1. These findings are correlating with the study of Lathi A et al [10] where the male to female ratio was 1.35:1. In the study of Dasgupta A7, male to female ratio was 1.91:1 and in Kulkarni A [8] study, male to female ratio was 2.25:1. In the study of Khan N et al [11] and Zafar U et al [4], male to female ratio was 1.7:1.
In the present study, the commonest complaint patient presented with was nasal obstruction. Out of 84 cases received, 68 (80.95%) complained of nasal obstruction. The second most common complaint was running nasal mass, 08 (9.52%) cases, followed by sneezing 5 (5.95%) and nasal discharge (3.57%). In other studies by Biswas G et al [9], Panchal L et al [12], Lathi A et al [10], Khan N et al [11], Kulkarni A et al [8] and Shah SN et al [13] Nasal Obstruction was the most common presenting complaint.
In the present study, most common Non-neoplastic lesion was Nasal Polyp comprising of 77 cases, followed by 2 cases each of Sinusitis and Intradermal Naevus. In other studies as mentioned in Table 2 commonest Non-neoplastic lesion was Nasal Polyp. In the study of Dasgupta A et al [7], Lathi A et al [10], Kulkarni A et al [8] and Kumari KMK et al [5], second most common lesion were Rhinosporidiosis. In the study of Nair S et al [14], cases of Sinusitis were more common than Polyp as the study was based on clinical findings.
In the present study, 77 out of 84 Non-neoplastic cases were Nasal polyps (91.6%). These finding correlate with the study of Biswas G et al [9] (90%), Lathi A et al [10] (87.5%), Khan N et al [11] (83.3%) Zafar U et al [4](82%), Bist SS et al [15] (78.1%). In the study of Nair S et al [14], the lowest percentage of nasal polyps (20.4%) were noted. (Table 3)
In the present study, inflammatory polyp (50 cases) was the most common among all polyps, followed by allergic polyp (20 cases). These findings were related with the other studies like Bakari A et al [16], where 35 cases were inflammatory polyp and 10 cases were Allergic polyp, Kumari KMK et al [5], where 35 cases were inflammatory polyp and 9 cases were Allergic polyp. In the study of Dasgupta A et al [7] and Lathi A et al [10], Allergic polyps were more than inflammatory polyps. Biswas G et al [9] and Nair S et al [14], noted Antrochoanal polyps only (Table 4).
CONCLUSION
In our study, most common lesions were Nasal Polyps. Most of the cases were presented in the 2nd and 3rd decade of life with male preponderance. Nasal obstruction was the most common clinical presentation in the present study.
REFERENCES
[1] Bosch ABV, Genaida F. Cancer of the Nasal Cavity. Cancer.1979; 37(II): 1458-63.
[2] Dawes JBD, Harkine DG, Marshall NP, Von Miert, PG. Malignant Disease of Nasopharynx. J. Laryng Otol. 1969; 85: 211-38.
[3] Sharmogratnam K, Sobine LH. Histological Typing Of Upper Respiratory Tract Tumours. International Histological Classification of Tumours 1978; 19.
[4] Zafar U, Khan K, Afroz N, Hasan SA. Clinicopathological study of Non-Neoplastic Lesions of Nasal Cavity andParanasal Sinuses. Indian J. of Pathol Microbiol 2008;51(1): 26-9.
[5] KalpanaKumari MK, Mahadeva KC. Polypoidal Lesion in Nasal Cavity. J.Clinical And Diagnostic Research 2013;7(6) :1040-42.
[6] Bruce MW. Tumors of Upper Respiratory Tract, Nasal Cavity, Paranasal Sinuses and Nasopharynx. In: Fletcher CDM. Diagnostic Histopathology of Tumours. Churchill Livingstone 2007:3rd Edi. 84.
[7] Dasgupta A, Ghosh RN, Mukherjee C. Nasal polyps-Histopathologic spectrum. IJO & HNS 1997;49(1): 32-37.
[8] Kulkarni AM, Mudholkar VG, Acharya AS, Ramteke RV. Histopathological study of lesions of nose and paranasal sinuses. IJO & HNS 2012; 64(3): 275-279.
[9] Biswas G, Ghosh SK, Mukhopadhyay S, Bora H. A clinical study of nasopharyngeal masses. IJO & HNC 2002; 54(3): 193-5.
[10] Lathi A, Syed MMA, Kalakoti P, Qutub D, Kishve SP. Clinicopathological profile of sinonasal masses: a study from a tertiary care hospital of India. Acta Oto rhinolaryngologica Italica 2011;31:372-7.
[11] Khan N, Zafar U, Afroz N, Ahmad SS, Hasan SA. Masses of nasal cavity, paranasal sinuses and nasopharynx : A clinicopathological study. IJO & HNS 2006;58(3):259-63.
[12] Panchal L, Vaideeswar P, Kathpal D, Madiwale CV, Prabhat DP. Sino-nasal epithelial tumors. J Postgard Med March 2005;51(1):30-4.
[13] Shah SN, Goswami Y. Study of Lesions of Nasal cavity, Nasopharynx and Paranasal Sinuses by Histological Examination. Gujarat Medical Journal 2012;67(2):70-2.
[14] Nair S, James E, Awasthi S, Nambiar S, Goyal S. A Review of the Clinicopathological and Radiological Features of Unilateral Nasal Mass. Indian J. Of Otolaryngol, Head Neck Surg 2013; 65(2):199-204.
[15] Bist SS, Varshney S, Baunthiyal V, Bhagat S, Kusum A. Clinico-Pathological Profile of Sinonasal Masses: An experience in tertiary care hospital of Uttarakhand. National Journal of Maxillofacial Surgery.2012;3(2):180-6.
[16] Bakari A, Afolabi OA, Adoga AA, Kodiya AM, Ahmad BM. Clinico-pathological profile of sinonasal masses: an experience in national ear care center Kaduna, Nigeria. BMC Research Notes 2010;3:186.
Table 2. Comparative Study of Incidence of Non-neoplastic lesions according to histopathological Diagnosis.
|
Diagnosis |
No. of Cases in Studies |
|||||||
|
Dasgupta A et al [7] (1997) |
Zafar U et al [4] (2008) |
Lathi A et al [10] (2011) |
Bist SS et al [15] (2012) |
Kulkarni A et al [8] (2012) |
Nair S et al [14](2013) |
Kumari KMK et al [5] (2013) |
Present study |
|
|
Sinusitis |
- |
5 |
- |
1 |
1 |
26 |
1 |
2 |
|
Mucocele |
- |
- |
2 |
- |
- |
4 |
- |
1 |
|
Intradermal Naevus |
1 |
- |
- |
- |
- |
- |
- |
2 |
|
Rhinosporidiosis |
55 |
- |
2 |
- |
14 |
3 |
2 |
1 |
|
Polyps |
110 |
119 |
70 |
53 |
70 |
9 |
44 |
77 |
|
Nasolabial Cyst |
- |
2 |
- |
1 |
- |
- |
- |
1 |
Table 3. Comparative Study of Incidence of Nasal Polyp in Non-neoplastic Cases.
|
Studies |
No. of Cases of Polyps per Non-neoplastic Cases |
% Cases of Polyps |
|
Biswas G et al [9](2002) |
9/10 |
90.0 |
|
Khan N et al [11](2006) |
120/144 |
83.3 |
|
Zafar U et al [4](2008) |
119/144 |
82 |
|
Lathi A et al [10]10 (2011) |
70/80 |
87.5 |
|
Bist SS et al [15] (2012) |
50/64 |
78.1 |
|
Nair S et al [14](2013) |
9/44 |
20.4 |
|
Present Study (2015) |
77/84 |
91.6 |
Table No. 4: Comparative Study of Incidence of Nasal Polyp According to Histopathological Diagnosis
|
Diagnosis |
No. of Cases in Studies |
||||||
|
Dasgupta A et al7 (1997) |
Biswas G et al9 (2002) |
Bakari A et al16 (2010) |
Lathi A et al10 (2011) |
Nair S et al15 (2013) |
Kumari KMK et al5 (2013) |
Present Study (2015) |
|
|
Allergic Polyps |
74 |
- |
10 |
50 |
- |
9 |
20 |
|
Inflammatory Polyps |
36 |
- |
35 |
20 |
- |
35 |
50 |
|
Antrochoanal Polyps |
- |
9 |
|
|
9 |
|
7 |
© Authors; 2019. International Journal of Clinical and Biomedical Research, Sumathi Publications.
This is an Open Access article which permits unrestricted non-commercial use, provided the original work is properly cited. (CC BY-NC-SA 4.0)
Int. j. clin. biomed. res. 2019;5(1):1-4.